Coronary artery disease remains a major health threat across Southeast Asia, with calcified plaque buildup presenting particular challenges for cardiologists seeking to restore blood flow to the heart. A breakthrough study led by Malaysian consultant cardiologist Datuk Dr Tamil Selvan Muthusamy promises to transform treatment options for patients with severely hardened arteries, a condition that has long frustrated medical professionals and complicated standard interventional procedures. The research, conducted by a team of local cardiologists, explores the potential of an innovative device designed to crack stubborn calcium deposits that resist conventional treatment methods.
Coronary artery disease develops when fatty deposits, cholesterol, calcium, cellular debris and fibrin proteins accumulate inside blood vessel walls over extended periods. These accumulations gradually narrow or completely block the affected arteries, progressively restricting oxygen-rich blood from reaching vital organs. Patients facing this progression confront escalating risks of heart attack, heart failure and stroke, making timely intervention essential. While lifestyle modifications and pharmaceutical treatments form the foundation of disease management, many patients ultimately require surgical or catheter-based procedures to restore adequate blood flow and prevent catastrophic cardiac events.
Standard interventional approaches employ several established techniques to address arterial blockages. Percutaneous coronary intervention, coronary artery bypass grafting and balloon angioplasty have proven effective for treating soft plaque accumulations by compressing fatty deposits and deploying stent devices to maintain arterial patency. However, these conventional methods encounter significant obstacles when confronting severely calcified plaque. As Dr Tamil Selvan explains, treating soft plaque remains straightforward—balloon expansion crushes the material to create adequate space within the vessel before stent placement prevents re-narrowing. The situation changes dramatically when calcium hardening transforms plaque into rock-like formations resistant to mechanical compression.
Severe coronary artery calcification represents an increasingly recognised clinical challenge that demands specialised techniques. Current therapeutic options include rotational atherectomy, high-pressure balloon angioplasty and intravascular lithotripsy, each capable of fragmenting calcium deposits and restoring blood flow. Yet these interventions remain fraught with technical difficulties, particularly regarding equipment delivery through narrowed vessels and achieving adequate stent expansion within calcified segments. Poor acute and long-term outcomes persist despite these advanced approaches, leaving cardiologists searching for superior solutions that combine efficacy with safety and reliability.
Intravascular lithotripsy represented a transformative advancement when introduced for treating calcified coronary disease. The procedure employs catheter-based systems that generate sonic pressure waves, fragmenting hardened calcium deposits within blood vessel walls. Despite its promise, however, the technology carries inherent limitations that constrain its clinical effectiveness. Existing IVL devices operate within fixed parameters—earlier generations permitted only eight ultrasound pulses to fragment calcium, while newer versions increased this to twelve pulses. This constraint means operators must accomplish complete calcium fragmentation within their pulse allocation, introducing planning complexity and potential treatment failures.
Device design constraints further compromise clinical utility. Current IVL catheters are relatively bulky, creating insertion difficulties when navigating severely narrowed coronary arteries with minimal remaining lumen space. Additionally, existing systems employ fixed balloon sizes, forcing clinicians to select a single diameter for vessels that vary significantly in width along their length. A coronary artery might measure 3.5 to 4mm in proximal segments, then narrow to 2 to 3mm distally, yet physicians must choose a single balloon dimension. This mismatch between device specifications and patient anatomy necessitates supplementary techniques and complicates procedural planning.
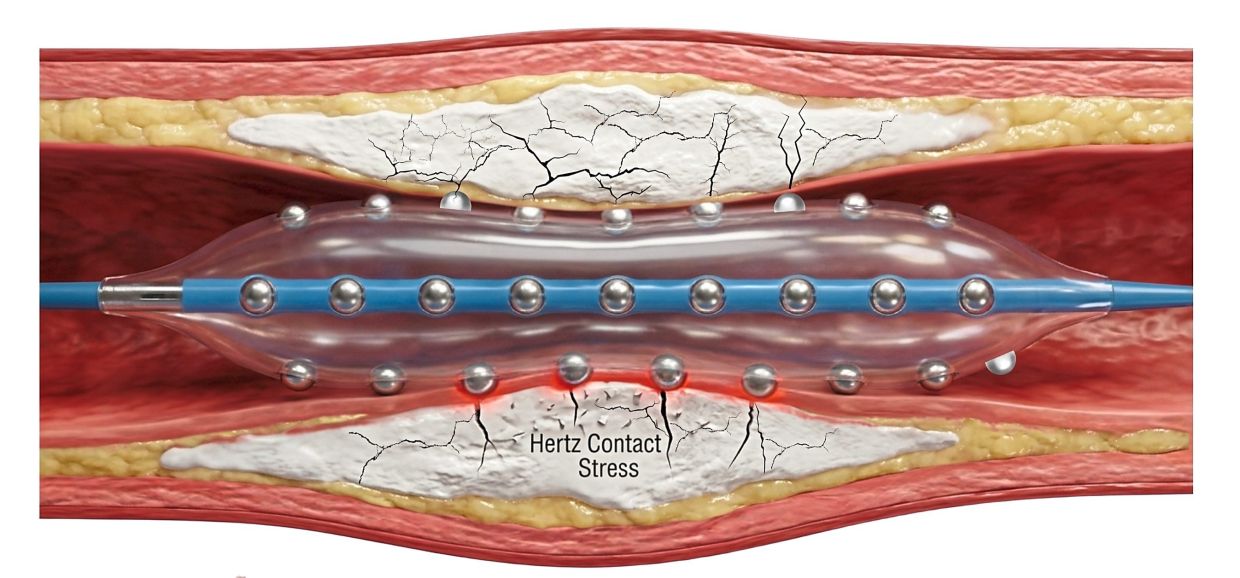
Recognising these limitations, Dr Tamil Selvan and his colleagues initiated investigation of the Hertz Contact-IVL System, an innovative variant specifically engineered to optimise expansion during percutaneous coronary intervention in calcified blockages. Unlike energy-dependent systems requiring external power generators, the HC-IVL employs a mechanical approach utilising integrated metallic hemispheres embedded within the balloon itself. When the device contacts calcium deposits under applied pressure, the hemisphere geometry amplifies and concentrates force specifically at the plaque interface, generating deep wide cracks that fragment rigid deposits without damaging surrounding arterial tissue. This mechanical principle permits effective calcium fragmentation through direct force transmission rather than external acoustic energy.
The HC-IVL design provides substantial practical advantages over existing technology. By eliminating dependence on external energy sources, the device becomes mechanically simpler and potentially more reliable. More significantly, improved catheter deliverability allows passage through narrowed segments with greater ease, enabling physicians to treat extended lesions or multiple vessels using a single balloon rather than requiring multiple device exchanges. This single-device capability reduces procedure duration, radiation exposure and contrast agent utilisation—important considerations for patient safety and procedural efficiency. The mechanical force amplification principle also eliminates the pulse-count constraints plaguing conventional lithotripsy systems.
The decision to conduct comprehensive local testing represented a strategic scientific judgment. Although the HC-IVL device developer had initiated early-phase investigations at multiple United States centres, those studies involved relatively small patient populations and limited data regarding safety profiles in diverse clinical scenarios. Dr Tamil Selvan recognised that robust validation required larger-scale investigation within a distinct patient population. Malaysian cardiologists possessed both the technical expertise and patient access necessary to conduct rigorous evaluation of device safety, efficacy and deliverability characteristics under real-world clinical conditions. This research would generate evidence supporting potential clinical adoption across Southeast Asia.
The implications of successful HC-IVL validation extend considerably beyond individual patient outcomes. Coronary artery disease remains endemic throughout Southeast Asia, with calcified plaque representing a particularly common presentation in this region. Enhanced treatment options for severely calcified blockages would expand interventional capabilities available to regional cardiologists, potentially reducing myocardial infarction incidence and improving survival rates among vulnerable populations. Malaysian institutions are positioning themselves as research leaders investigating innovative solutions to prevalent regional health challenges, potentially establishing frameworks for future therapeutic evaluations and clinical adoption pathways.
Successful adoption of advanced lithotripsy technology requires not merely technical efficacy but genuine improvement in clinical outcomes and procedural safety. The HC-IVL system's mechanical design offers theoretical advantages regarding reliability, deliverability and versatility compared to existing energy-based systems. However, comprehensive clinical validation remains essential before widespread implementation. The Malaysian research team's commitment to rigorous study methodology reflects appropriate scientific caution, ensuring that any subsequent clinical adoption rests upon solid evidence rather than preliminary enthusiasm.
As cardiac disease prevention and treatment remain critical health priorities throughout Southeast Asia, innovations addressing treatment-resistant presentations deserve serious attention. The work undertaken by Dr Tamil Selvan and his colleagues represents precisely this investigative approach—examining whether emerging technologies offer genuine clinical advantages for patients facing life-threatening arterial blockages. Positive results could meaningfully expand therapeutic options for regional cardiologists and ultimately improve outcomes for countless patients confronting coronary artery disease in Malaysia and throughout the broader Southeast Asian region.

